SIGforum.com  Main Page The Lounge Socio-Capitalist Healthcare Systems Around the World (Coronavirus Spin-Off)
Main Page The Lounge Socio-Capitalist Healthcare Systems Around the World (Coronavirus Spin-Off)
The Lounge Go | New | Find | Notify | Tools | Reply |
| SIGforum's Berlin Correspondent  |
As noted on the main Wu-flu thread with its recurring debates on how different systems are able to respond to crises:
Some background on the local system. Germany has two-tier health insurance. The first tier is statutory insurance, which was the first of the public welfare schemes introduced by Bismarck from 1883 to cut the ground from under the feet of socialist movements. Enrolment is generally mandatory for anybody who can't provide for his healthcare by other means. Contributions are paid 50:50 by employee and employer (or social insurance for unemployed, the public retirement fund for retirees, etc.), currently 7.85 percent of the wage respectively, with some variations over the years. Non-working spouses and kids up to age 18 (25 for students) are co-insured. Insurees must chip in a little for prescription drugs (usual five or ten Euros depending on type and package size) and dental replacement. The insurances are responsible for their own budgets and can demand limited extra contributions beyond the legally mandated rate, but must pay for a defined list of services. Since 2009, payments are no longer direct from insuree to insurance, but are distributed via a national health funds which also gets some federal money for services beyond the strict scope with which the government has tasked insurances. The second tier is private insurance, for which anybody beyond a certain income threshold (currently 62,550 Euro per year) is eligible; or people just can drop out entirely and pay for their own health cost, which about 0.2 percent of the German population do. Private insurers set their own premiums, depending on the insuree's health status (and they can reject people depending upon pre-existing conditions), though employees are still being paid an allowance corresponding to the 7.85 percent of their wage by the employer. Self-employed pay in full, of course. Private insurance may include additional services beyond the legal scope, and their insurees are generally treated preferentially by doctors; mostly because they get their money faster. Getting an appointment can be much quicker than with statutory insurance. Some doctors treat private patients exclusively, in part because you cannot just open a practice accepting statutory insurance anywhere but have to get a slot allocated to certain areas by the respective state's association of statutory health insurance physicians, self-regulatory organizations overseeing supply and competition of medical services. Still, there tends to be an abundance of GP and specialist practices in urban areas, while it's hard to get and hold doctors in rural regions with dwindling populations. My goal was long to make enough to become eligible for private insurance; but when I finally did I didn't switch, prefering to pay for extra services with my own money, because there are some pitfalls. Private premiums rise with age, and if your income drops, you may no longer be able to pay them, while statutory insurance won't take you back after more than five years if you're over 55. The line is also blurred because statutory insurers offer additional services for extra money. A problem for them is that private insurance tends to snap off the young and healthy, while they have to take anybody, with corresponding higher cost at legally fixed contributions. The political left has of course long demanded to switch to a unified statutory system and abolish "two-class medicine". The cost, or rather payment of individual medical services by statutory insurance are negotiated via the Joint Federal Committee of insurers, doctors, dentists, therapists and hospital operators (unified in 2004 from previous separate committees for the different fields). Insurers also strike their separate deals with drug suppliers. As for the meat of this topic, hospital cost are set by an institution under commercial law involving the national associations of statutory insurers, private insurers and hospital operators established in 2001. Previously, stationary hospital services were paid for via day rates for time spent in-house by the patient at 80 percent, the rest via case rates and individual payments for specific treatment. By the Millenium, it was becoming obvious that the traditional German healthcare/welfare system was becoming unsustainable due to a ageing population with less contributors and more recipients. The growing senior age bracket also needed more and longer medical treatment (which of course in turn made them live even longer). German hospitals were criticized for being cost-ineffective because patients were spending too much time in them. So the system was changed as part of the post-millenial welfare/healthcare reforms under chancellor Gerhard Schröder (which started the decline of his Social Democrats as disgruntled leftwingers abandoned them). The new basis were Diagnosis Related Groups (DRGs), originally developed by US hospitals as a patient classification system and later adapted for cost determination purposes; i. e. hospitals don't get paid mostly for the time a patient spends in the house, but lump sums based upon what is considered necessary to treat specific diagnoses. The German G-DRG system was adapted from Australia specifially and became effective in 2003. This forces hospitals to treat patients as economically, and discharge them as quickly, as possible, or they will lose money on them. As a result, staying times and hospital bed capacity in general have gone down, mostly by closing smaller houses, often in the course of operators being taken over. At the same time, just like in the US the number of ICU beds has actually risen (from 23,000 in 2007 to 28,000 in 2017, currently at 79 percent capacity). It has also saddled hospitals with a greater administrative burden, increased by refinement of DRG keys to match variations in diagnoses to necessary treatment cost. Generally, it has been criticized as commercializing healthcare and letting the market dictate treatment; though I'm not sure if there is a better solution for a system that provides as excellent care by international standards as the German, but with the associated cost and under the ambient demographic conditions. Ressources: OECD numbers for hospital beds per capita, by country Growth of critical care beds in the US Critical Care Bed Capacity in Asian Countries and Regions Variability of critical care beds in Europe 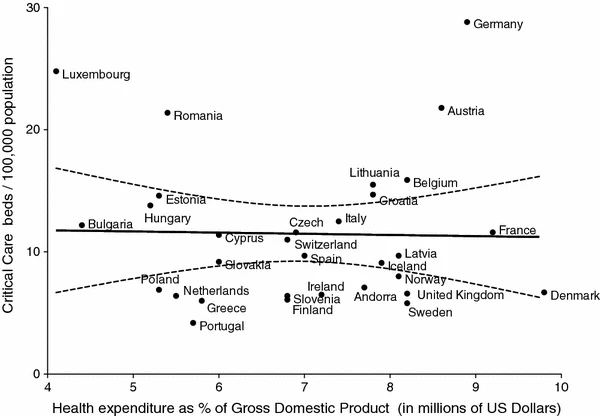 (2012 numbers) | ||
|
| SIGforum's Berlin Correspondent |
Also just found this report which is very apropos, thought it comes with the "Spiegel"'s left-wing slant.
https://www.spiegel.de/interna...bb-8caf-8f6074e641cf | |||
|
Member |
Here's another perspective. https://mises.org/wire/markets...PajuLWAwKEtNwVvYYgcw ----------------------- Markets vs. Socialism: Why South Korean Healthcare Is Outperforming Italy with COVID-19 Everyone is vitally aware of the spread of the novel COVID-19 pandemic as it rages in early stages across the globe. Travel restrictions are everywhere as people are trying to get tested, prepare for possible quarantines, and worrying about their jobs and their families. Events involving large groups of people are canceled, and in some cases entire countries are being locked down. But in all this flurry of reaction over the crisis, there is an almost natural experiment in how well a socialized healthcare system can respond to such a problem. And the answer appears to be…not well. To demonstrate, we can look at the two cases of Italy and South Korea. As of the time of this writing (3/12/2020), Italy has experienced 15,113 cases while South Korea has confirmed 7,869. However, the South Korean number is rising at a relatively tepid ~100 cases a day to Italy’s roughly 2,500 added today. (Data on the spread of the novel coronavirus was obtained from this site tracking the outbreak.) Overall, Italy and South Korea have similar populations (around 60 million and 50 million, respectively), although the South Korean half of the Korean Peninsula is about a third of the size of Italy in terms of land area. Italy is experiencing a quickly spiraling exponential growth in confirmed cases despite shutting down the entire country with curfews and travel restrictions and heavily focusing on the provision of care. By contrast, even with a cult that essentially spread the disease on purpose, South Korea has gained a strong foothold in containing COVID-19. There are many reasons for this difference in outcome, but some of them are directly related to the far more socialized healthcare system in Italy. South Korean Healthcare Although South Korea does have a state-monopolized system providing a universal health insurance, this state-provided insurance is not able to set prices in the market for healthcare. Hospitals and clinics routinely charge patients more than the state insurance will pay, which has caused many Koreans to take out private insurance to cover the difference. TheKorea Bizwire reports that eight out of ten Koreans take out such insurance, with the average Korean paying just over 120,000 won (about $120) a month for it. Care is provided by a set of hospitals that are 94 percent privately owned, with a fee-for-service model and no direct government subsidies. Many of these hospitals are run by charitable foundations or private universities. Private hospitals in the country exploded in number from 1,185 in 2002 to 3,048 in 2012. The result is that South Korea has 10 hospital beds per 1,000 people, more than twice the Organisation for Economic Co-operation and Development (OECD) average (and nearly three times as many as Italy’s 3.4 beds per capita). These private hospitals also charge significantly less (between 30–85 percent of the price) than US hospitals (which are also often required to get a “certificate of need” from the government before construction, depending on what state they are built in). Italian Healthcare In Italy, by contrast, surgeries and hospitalization provided by public hospitals or by conventional private ones are completely free of charge for everyone regardless of their income. This is entirely paid for by the the national health service, the Servizio Sanitario Nazionale (SSN) (as are family doctors' services). Waiting times can be up to a few months for large public facilities, though they are somewhat shorter for small private facilities with contracts to provide services through the SSN. Public and private medical providers offer “free market” options in which the patient pays directly, but this is rarely taken up and thus contributes very little to hospital revenues. Emergency medical service is always free of charge. Italy experienced an ongoing health worker shortage even before COVID-19 struck the country. The number of hospitals in the country has been on a steady decline over the last couple of decades, from 1,321 in 2000 to 1,063 in 2017. SSN prices for payments to hospitals were set below market rates for the purpose of saving money on healthcare, and the results were as expected for a de facto price control. Conclusion Currently, the Italian healthcare system is overwhelmed by the tens of thousands of COVID-19 cases it is already facing. They have turned to rationing care to prioritize the young, leaving those most at risk of the virus to essentially fend for themselves. Most just chalk this up to the severity and danger of the pandemic. However, the evidence tells a different story. It portrays a situation made far worse by a reliance on government-centralized healthcare that manages costs by de facto price rationing rather than a free market system. Although South Korea provides a basic safety net, it is also one of the closest healthcare systems in the world to a free market, outpacing to a significant degree even the US system (which includes a great number of supply-restricting regulations that only drive up costs and hurt availability). As a result, South Korean healthcare did what Italy’s already undersupplied system could not do—cope effectively with the pandemic and manage to get it under control without shutting down the entire country in the process. If US officials wish to effectively handle the rising number of cases in big cities, they would do well to take lessons from South Korea and start freeing the market for healthcare rather than bungling a monopolized testing protocol that did not need to be monopolized, and thereby preventing people from getting tested. This would not immediately resolve the problems created by bad regulation in the past, but it would certainly reduce its negative consequences while improving the healthcare system's ability to deal with these sorts of crises going forward. It would also have the benefit of reducing the cost of healthcare generally. . | |||
|
Member |
Tagged for use. ========================================== Just my 2¢ ____________________________ Clowns to the left of me, Jokers to the right ♫♫♫ | |||
|
| Member |
The lessons you list in the 2nd article are pretty much was my physician of 23 years told me as we talked about health care in this country. I read a piece in the WJS 20 years or so back talking about how the private sector health care system here was moving toward rationing health care. People here might be surprised to learn how many H1B's are medical related - especially in Texas. Of course these foreign Physicians make more here than in their home country's socialized medicine world, but also forces them to do certain things to keep their H1B status (like pushing pills for the legal drug pimps in the U.S.). For my last colonoscopy, the facility was not too happy with me, as I took too long to come out of anesthesia - taking up a bed longer than proscribed in the industrial assembly line process in place for this procedure. And after I came out, I was a tad woozy - BP of 101 over 74, but got kicked out regardless. I was ok 10 minutes later. To me today, there really is no significant difference between private and public health care. They both ration services. Germany's health care is not what it was once when my mother used it before the leaving in '69. Don't even launch her about medical care / private insurance in this country. PS: I still remember standing in lines with my school mates in West-Berlin '68 or '69 and getting our mandated immunization(s) (Impfungen) for what ever. Somewhere I think I still have my WHO Impfung Buch. -.-. --.- -.-. --.- -.-. --.- -.-. --.- It only stands to reason that where there's sacrifice, there's someone collecting the sacrificial offerings. Where there's service, there is someone being served. The man who speaks to you of sacrifice is speaking of slaves and masters, and intends to be the master. Ayn Rand "He gains votes ever and anew by taking money from everybody and giving it to a few, while explaining that every penny was extracted from the few to be giving to the many." Ogden Nash from his poem - The Politician | |||
|
| Member |
Healthcare here in the US isn't really private. Medicare drives much of the policy and the quasi-governmental oligopoly of medical insurance does the rest. Hospitals are jumping to their tunes, because they own the revenue stream. . | |||
|
| Powered by Social Strata |
| Please Wait. Your request is being processed... |
SIGforum.com Main Page The Lounge Socio-Capitalist Healthcare Systems Around the World (Coronavirus Spin-Off)
The Lounge © SIGforum 2026